Keywords: Palliative Care
-

AUSTRALIA
- Annmarie Hosie
- 25 May 2021
27 Comments
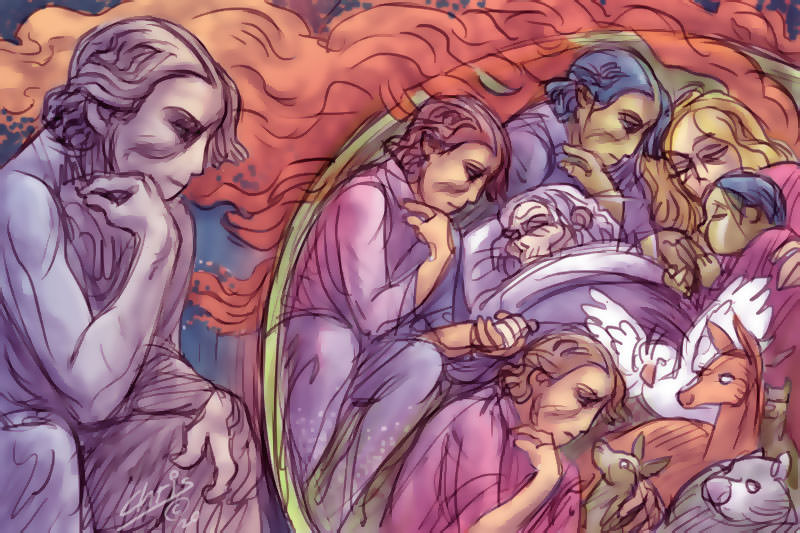
Peace, laughter and lightness during dying might seem unlikely, but such experiences are common, not rare. Seeing and sharing in these sudden, strengthening consolations (and receiving them in my own griefs) have taught me about our awesome potential to transcend suffering, and confirmed why we don’t need euthanasia or assisted suicide.
READ MORE 
-

AUSTRALIA
- Frank Brennan
- 20 May 2021
25 Comments
Australian jurisdictions are presently considering laws and policies relating to euthanasia, physician assisted dying and medically assisted suicide. The law can and should provide bright-line solutions or at least firm parameters within which the dying, their loved ones and their care providers can negotiate dying and death.
READ MORE
-
AUSTRALIA
- Jenneke Foottit and Sue Gledhill
- 11 March 2021
2 Comments
The recently released report of the Royal Commission into Aged Care does not hold back in describing a situation that should be abhorrent to us all. As the report notes, ‘substandard care and abuse pervades the Australian aged care system’.
READ MORE
-

AUSTRALIA
- Justin Glyn
- 10 September 2020
9 Comments
While the legislation was proposed as something of a measure of last resort, the numbers already tell a different story. Unfortunately, many of us with a disability look at these figures (and at the proposed legalisation of euthanasia in New Zealand, which will be voted on later this year) with a weary mix of familiarity and horror.
READ MORE
-
ARTS AND CULTURE
- Julie Perrin
- 06 April 2020
4 Comments
While I stay by my mother, I glean only the edges of the news; already the horror of the fires has been at full stretch. In the quiet room where my mother lies, I think of people trying to sleep in unfamiliar environments, refugees from the fires.
READ MORE
-

ARTS AND CULTURE
- Katherine Richardson
- 26 September 2019
8 Comments
Before that first September, my experience with grief was fairly limited. I was no stranger to death, but I hadn't yet felt the type of grief that makes you ache in places you never realised sadness could reach. My first experience with this was September 2014.
READ MORE
-

ARTS AND CULTURE
- Maureen O'Brien
- 20 March 2019
14 Comments
On the morning of your last day there are eight people, including me and my daughter, who is a music therapist and has played music for people as they die as part of her clinical practice. After discussions during the week, first with you and then with your neurologist, it was decided that she will sing for you and the people with you today.
READ MORE
-

RELIGION
Assisted suicide is not just a matter of being given a 'choice'. There is a whole system that would need to be created, with hospitals, doctors, nurses, lawyers, politicians and families all involved in facilitating this choice. Should we be enlisting the liberty of all these people to facilitate this choice?
READ MORE
-

RELIGION
- Hoa Dinh
- 22 September 2017
22 Comments
Euthanasia legislation would lead to further coercion against vulnerable persons in society: the elderly and people with disability. Once voluntary suicide is legalised, to continue living becomes a choice that people will have to justify to themselves, their family, and society. It is especially the case for persons who have to depend on the assistance of others: the elderly, and people with disability.
READ MORE
-

AUSTRALIA
- Kate Moriarty
- 10 March 2017
51 Comments
I'm what you might call a feminist outsider. I'm passionate about the rights of women. I believe every girl should have the opportunity to be educated, and that workplaces need to become more accommodating of families. I spend a worrying amount of time shouting 'You wouldn't say that if she were a man!' to commentators on the radio. I'd like to be called a feminist. But I don't think I'm allowed to be. You see, I also believe a baby is a person before she is born. And I believe that person has rights.
READ MORE
-

RELIGION
- Frank Brennan
- 03 December 2015
The consideration of medico-legal problems in the public square of a pluralistic democratic society keeping pace with profound technological change is often marked by simplistic assertions, precluding considerations of comprehensive world views, whether religious or philosophical. It is now commonplace for doctors to be told to leave their consciences at the door, as their patients are consumers and they are suppliers and of course the market decides. Debates about law and policy are often resolved with simplistic assertions about individual rights and autonomy, with little consideration for the public interest, the common good, and the doctor-patient relationship. Even conscience is said to be a matter for contracting out. This evening I ask whether there are more compelling ways to resolve medico-legal dilemmas, while conceding a limited role for law in determining the range of acceptable answers.
READ MORE
-
RELIGION
- Frank Brennan
- 27 November 2015
2 Comments
'The crisis of child sexual abuse in our societies has required that our institutional procedures be more transparent and that we learn from the ways of the world in exercising power openly and justly. This means we have to restructure some of our church arrangements so that power is exercised accountably and transparently. All of us who have positions of influence and power in institutional churches need to be attentive to the voices of those who have suffered within our institutions.' 'Discerning the place for the prophetic voice and pragmatic cooperation of the churches in the great moral questions of the age', address to the Association of Practical Theology in Oceania conference, 26 November 2015.
READ MORE